Spondyloarthritis
#Bewegingsstelsel #Rheumatologie
Spondyloarthritis is meer dan spondylosis ankylosans! Het betreft een heel spectrum met klinische overlap tussen de verschillende ziekten in het concept
Symptomen
Inflammatoire perifere arthritis
- oligoarticulair (prototype)
- assymetrisch
- vooral grote gewrichten OL
- inflammatoire pijn
- bewegingsbeperking
Enthesitis
- vrl hiel en OL
- thv insertie pezen, ligamenten …
Testen
Rx of MRI
- sacroillitis +/- spondylitis
Labo
- associatie met HLA-B27
- afwezigheid van RF
- inflammatoire parameters (CR, ERS)
Goede respons op NSAID’s
Geschiedenis
Familiale geschiedenis
Voorgaande infecties
Spondylitis ankylosans |
Psoriasis arthritis |
Reactieve arthritis |
IBD arthritis |
|
|---|---|---|---|---|
Gender (M/F) |
3/1 | 1/1 | 8/1 | 1/1 |
Age of onset |
<40 | Kan op elke leeftijd (piek op 20j) | 20-40 | 20-45 |
Target therapies |
IL-17, anti-TNF | IL-17, IL-12/23, anti-TNF (etanercept minder effectief) |
anti-TNF | IL-12/23, anti-TNF (geen etanercept) |
Eigenschappen |
Symmetrisch 90% HLA-B27 positief Vaak uveïtis Bijna altijd axorillitis/spondylitis |
Asymetrisch Kan elk gewricht aantasten |
Asymmetrisch 70% HLA-B27 positief Vaak uveïtis |
Symmetrisch OL |
Predominant axiale SpA
Spondylitis ankylosans
-
Wat?
Progressieve, chronische, inflammatoire, reumatische aandoening
- typische inflammatory back pain, met ook perifere en extra-articulaire aantasting
- kan ankylose geven sacroilliacale gewrichten & wervelzuil
- M/V → 3/2
- 0,5-1%
- jonge patiënten, meestal <40j
-
Pathogenese?
Samenspel van genetische, externe en interne triggerende factoren
Genetisch
HLA-B27- belangrijke genetische factor
- noch noodzakelijk, noch voldoende voor ontwikkelen SpA
Zeker nog andere genen betrokken
Extern
InfectieMechanische stress
Intern
Gut dysbiosisMicrodamage
-
Kliniek?
Beoordeling ziekteactiviteit via**BASMI**- cervicale rotatie
- tragus(oor)-muur afstand
- lateroflexie (afh van leeftijdsgroep)
- schöber index (lumbale flexie)
- intermalleolaire afstnad
- thoraxexpansie
Classificatie-criteria
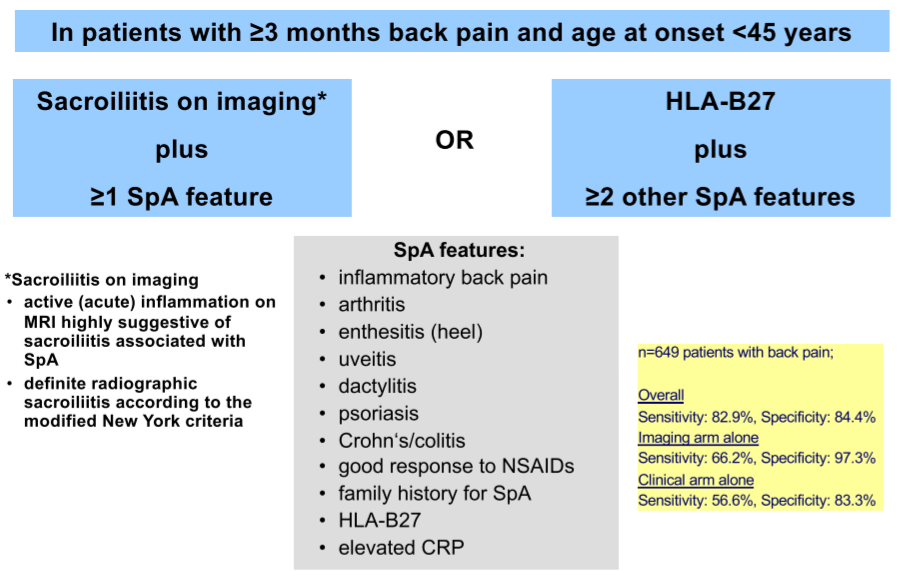
→ zowel perifere (>35%) als extra-articulaire aantasting -
Diagnose?
Non-radiographic stage
Bloedwaarden tonen verhoogd CRPRadiographic stage
Syndesmophyten (differentiatie met degeneratieve rugziekte - osteofyten)Sacroillitis
Vernauwing gewrichtsspleet tot ankylose
Erosies, sclerose
Beiden verhogen risico op spinal radiographic progression
**Liefst voor radiographic stage al een diagnose **
-
Behandeling?
Niet-medicamenteus
Actief oefenen! (SMART)Sportbeoefening
Lokale warmte, massage… (enkel om beter te kunnen oefenen)
Medicamenteus
NSAID’s- best continu geven
→ remt evolutie (spinal radiographic progression)
→ vermindert cardiovasculair risico
(DMARDs)
Biologicals
- TNF-blokkers, anti-IL17, JAK-inhibitoren…
- in case of insufficient NSAID response
- monotherapie ↔ RA
- best continu geven
-
Complicaties?
- meest frequente comorbiditeit was osteoporose (13%)
- gevolgd door gastroduodenale ulcera (11%).
Predominant perifere SpA
Reactieve arthritis
-
Wat?
Acute arthritis, secundair aan infectie op afstand
- geen micro-organisen in gewricht
- meestal mono-arthritis, vooral OL
- in opstoten, goede prognose
- jonge patiënten, meestal 20-40j
**=/= septische arthritis **
-
Pathogenese?
Wegens secundair op intitiële infectie op afstand → gastheerreactie belangrijk voor pathogenese -
Behandeling
- NSAID
- Intra-articulaire corticosteroïden
- DMARD’s (sulfasalazine)
- AB
- geen relevant effect op arthritis
- wel voor primaire infectie
- Anti-TNF therapie
Psoriatic arthritis
-
Wat?
Psoriasis geeft verhoogde kans op inflammatoire arthritis
- kan op elke leeftijd, maar piek op 20j
- M/V → 1/1
- meest frequent plaque psoriasis
**Nog veel andere psoriasis-related co-morbidities: - crohn- uveitis- anxiety/depression- metabool syndroom- cardiovasculair **
-
Pathogenese?
Ontwikkelt meestal bij reeds bestaande psoriasis (70-80%) (a priori vs a sine)
-
Kliniek?
5 typische presentaties- Asymmetrische mono-/ oligoarthritis
- Symmetrische polyarthritis
- Distal interphalangeal (DIP) joint involvement
- Axiaal IBP (spondylitis and sacroiliitis) (HLA-B27)
- Arthritis Mutilans
Dactylitis & enthesitis ook frequent
-
Diagnose?
Vooral patroonherkenning klinisch
Daarnaast labo:- zelden RF of anti-CCP
- acute fase merkers (ESR,CRP) kunnen verhoogd zijn
- hyperuricemie
-
Behandeling?
- Methotrexaat
- 15mg/w (escalatie tot 20mg/w)
- oraal/IM/SC
- monotherapie of anker in combinatietherapie (met DMARD’s bv)
- foliumzuur associëren & follow-up transaminasen (levertoxiciteit)
- DMARD’s (bij bevestigde arthritis)
- leflunomide
- NSAID (for symptomatic bridging treatment)
- Biologicals zoals anti-TNF (indien methotrexaat niet effectief)
- etanarcept minder effectief
- bij voorkeur biofarmaca in associatie met methotrexaat
- Methotrexaat
IBD arthritis
-
Wat?
IBD met musculoskeletale manifestaties
- 20-45j
- M/V → 1/1
-
Kliniek?
Klassieke GI symptomen: diarree, abdominale pijn, koorts, gewichtsverlies, fistels…
Perifere manifestaties12-30%
HLA-B27 niet verhoogd
Pauci-articulair, assymetrisch, OL
Neemt toe met ziekteduur
Dactylitis, enthesitis en clubbing (→ enkel bij IBD)
Axiale manifestaties10-20%
HLA-B27 verhoogd
Vergelijkbaar met klassieke SA
Evolutie onafhankelijk van darmaantasting**Vertonen zelfde patroon als de andere SpA **
-
Behandeling?
Gastro-intestinaalCorticoïden
Basistherapie
- 5-ASA
- Azathioprine
Biologicals (anti-TNF, anti-IL12/23, anti-integrines, JAK-inhibitoren)
ArticulairNSAID?
Salazopyrine?
Biologicals (anti-TNF, anti-IL12/23, JAK-inhibitoren) (etanercept niet bij Crohn)
Extra-articulaire manifestaties
SpA concept gerelateerd
Oog - Huid - Darm - Urogenitaal
- Frequent (20-60%)
- Klinische inflammatie
- Kan op elk ogenblik tijdens ziekte evolutie
- Soms gerelateerd aan locomotorische aantasting
- Klassieke SpA behandelingen werken
→ effect van TNF-blokkers!!
Niet-SpA concept gerelateerd
Long - Nier - Hart - Zenuw
- Zeer zeldzaam (1%)
- Meestal subklinisch
- Meestal pas laattijdig
- Niet gerelateerd aan locomotorische aantasting
- Geen effect van klassieke SpA behandelingen
→ effect van TNF-blokkers??
Clinical presentation of patients with SpA is crucial in therapy choice