Kalium
Hypokaliëmie
Diagnostische work-up
1. Extra-renaal
Urinair K+ <15mmol/dag
- GI verlies (>>)
- diarree
- laxativa
- villeus adenoma
- Onvoldoende inname
- Perspiratie ++
2. Renaal
Urinair K+ > 15mmol/dag
- Tubulaire acidose
- Keto-acidose
- Cl- depletie (metabole alkalose)
- braken/maagaspiratie
- diuretica
- Bartter/Gitelman syndroom
- hyperaldosteronisme
- mineralocorticoïd excess (incl zoethout)
- Farmaca
- antibiotica
- amphotericine B
- Polyurie
- Hypomagniësemie
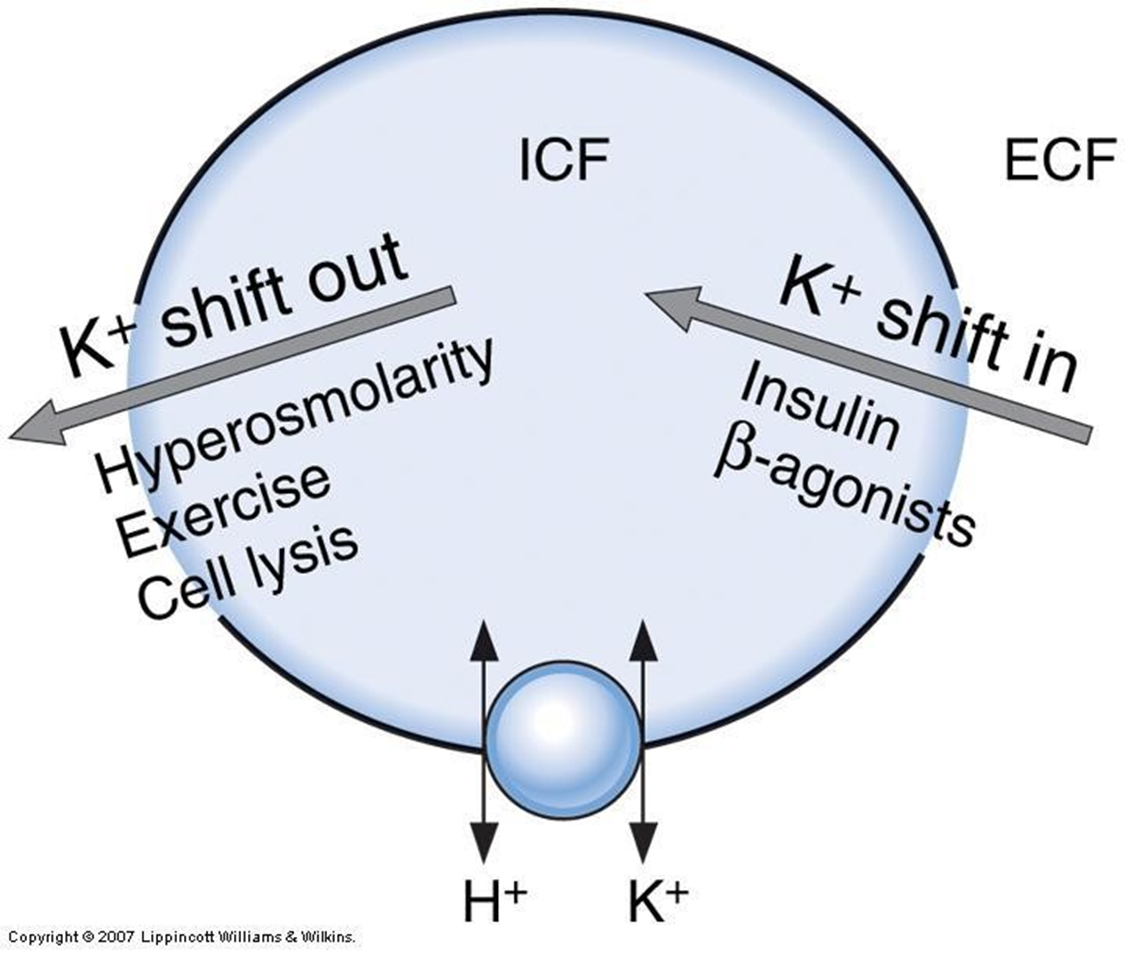
3. Trans-cellulaire shift
- Alkalose / corrigeren van acidose
- Insuline tediening of excess (exogeen/endogeen)
- Beta-adrenerge catecholamines
- stress
- beta-agonisten (bronchodilatoren)
- Intoxicaties
- theofylline
- tolueen
- Hypothermie
Acidose en insuline-deficiëntie verhogen kaliëmie
Therapie
Inname
- Extra K PO/IV
Uitscheiding
- stop K-verlagende medicatie
- behandel hyperaldosteronisme
- start kaliumsparende diuretica evt
- magnesium mag je standaard opstarten
Als U-golf > T golf amplitude is serum K < 3 mEq/L
HypoK vrl gevaarlijk bij hart- en vaatziekten
Hyperkaliëmie
Diagnostische work-up
1. Verhoogde inname
- Groeten, fruit, vervangzouten
2. Gedaalde urinaire excretie
- Hypo-aldosteronisme /
- Medicatie
- ACE-I & ARB
- co-trimoxazole & NSAID
- aldosteronatagonisten (spironolactone)
- Ernstie nierinsufficiëntie
- Deshydratatie
3. Trans-cellulaire shift
- Acidose
- Insulinetekort
- Celkatabolisme
- trauma
- crush syndrome / rhabdomyolyse
- Hemolytisch bloedstaal
- Beta-blokkade
- Digitalis intoxicatie
Therapie
HYPERKALIËMIE IS EEN URGENTIE
- hartritmestoornissen
- nood aan cardiale monitoring
- spierzwakte
- Ca-gluconaat
- beïnvloedt niet K maar wijzigt depolarisatiedrempel hartcellen, beschermend effect, minder snel hartritmestoornissen
- Hypertone glucose met insuline IV
- monitoring glycemie elke 4-6u CAVE hypo's
- transcellulaire shift
- NaHCO3 IV
- transcellulaire shift
- Kayexalate PO/rectaal
- gaat opname K in darm tegen
- Stoppen met K-verhogende medicatie
- Dialyse