Focale Leverletsels
Levercyste |
Hemangioom |
FNH |
Leveradenoom |
Levercarcinoma |
|
|---|---|---|---|---|---|
Wat? |
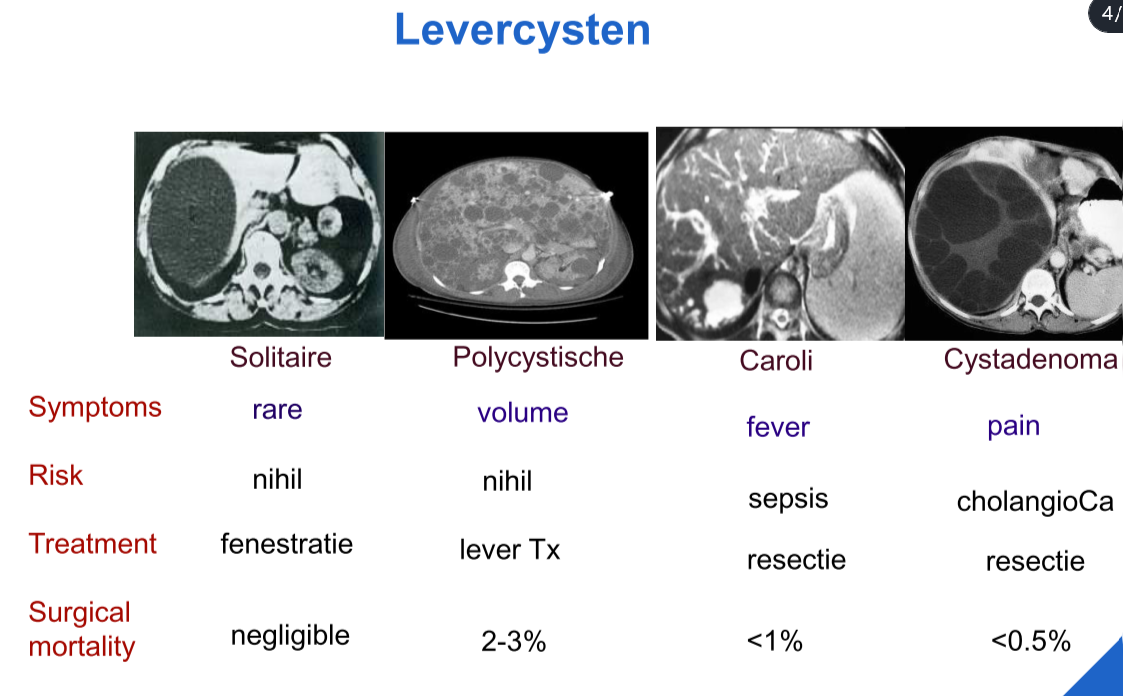
Dunne fibrotische wand (eenlagig cuboid epitheel) Bevat helder vocht Soms deel van erfelijke vorm van polycystose Geen risico op ontaarding |
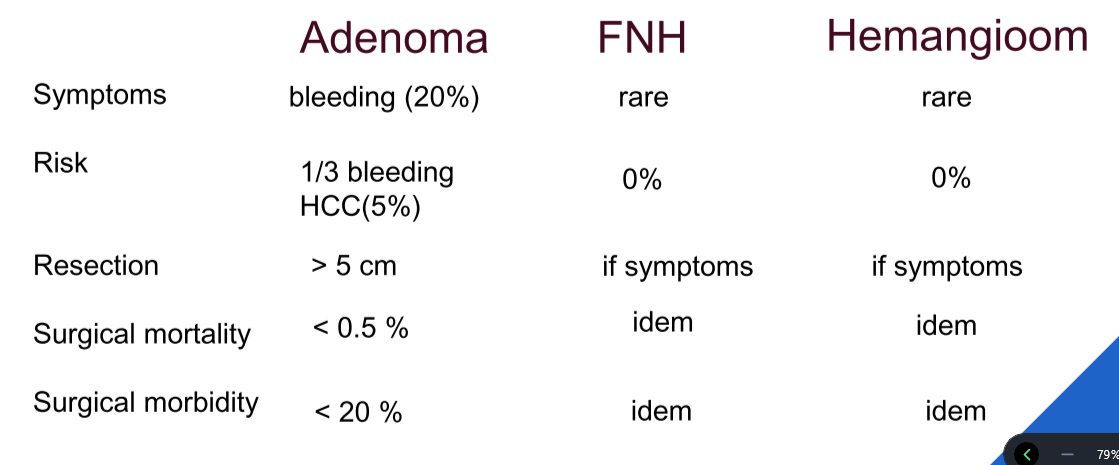
Frequentste benigne levertumor Stabiel letsel zonder maligne potentieel) Goed omschreven letsel (afgelijnd met endotheel, ondersteund door fibreus stroma) Meestal <3cm, vooral bij vrouw |
Benigne niet-omkapselde tumor Hyperplastische reactie op abnormale bloedtoevoer Vooral bij vrouw Geen relatie met OC (itt leverceladenoom) Geen maligne potentieel |
Niet-omkapselde, meestal solitaire tumor Vooral bij jonge vrouwen met OC (>5j) Wel maligne potentieel (5%) - type leveradenoom bepaalt risico op ontaarding of complicaties >10 → adenomatose |
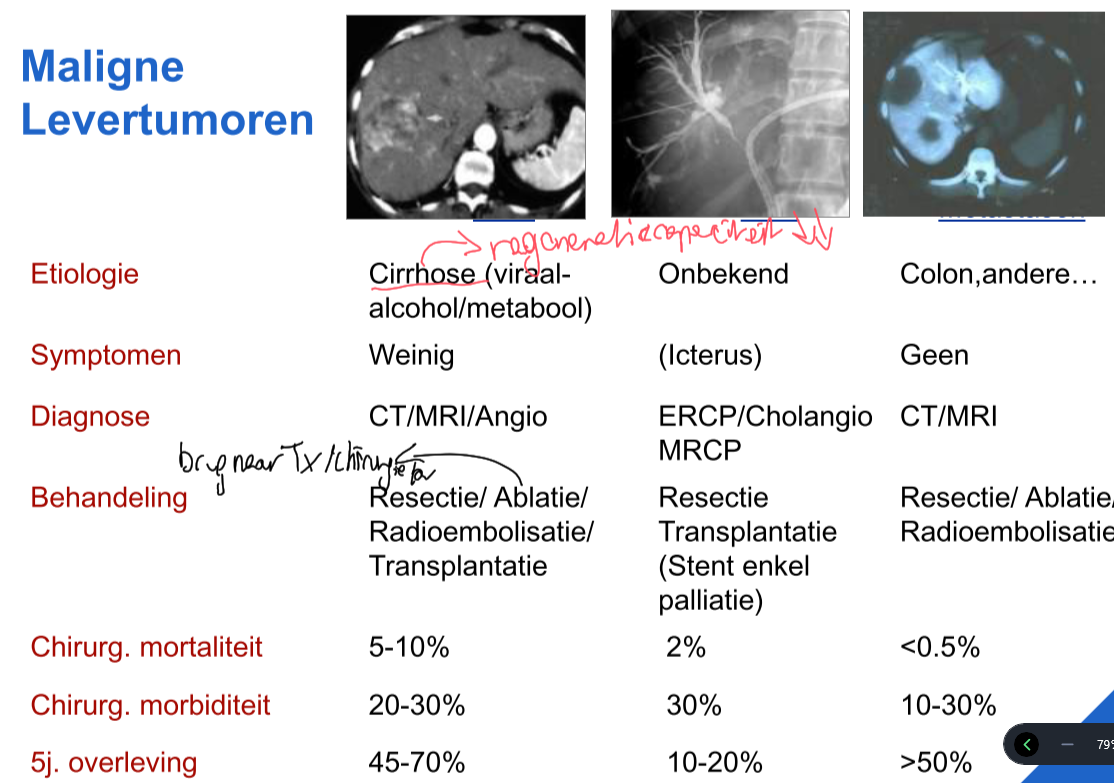
6de meest frequente ca (en stijgende) 90% onderliggende cirrhose (alcohol, NASH, hep B & C, mycotoxines) Metastaseert intra- en extrahepatisch Bijzondere geografische spreiding Toename in frequente in onze streken |
Symptomen |
Asymptomatisch → meestal toevallige diagnose bij echo of CT Pijn rechter hypochondrium Volume/massa effect Zelden bloeding |
Asymptomatisch Zelden bloeding of ruptuur |
Asymptomatisch | Asymptomatisch Hepatomegalie Pijn rechter hypochondrium Verwikkelingen (bloedingen 20%, ruptuur) |
Hepatomegalie Pijn rechter hypochondrium Koorts Beginnende icterus Gewichtsverlies Refractaire ascites |
Onderzoek |
Echo of CT ! kwaadaardige tumoren kunnen levercysten nabootsen, wegen uitgesproken centrale necrose ! |
Echo (welomschreven hyperechogene zone) MRI (diagnostische zekerheid) |
Echo MRI (diagnose) |
Echo (screening) MRI (diagnose) |
Echo (ook punctie) CT-scan MRI Doppler (invasie v. porta?) |
Labo |
Normaal/gestegen AF en gamma-GT (wegens druk op galwegen) Alfa-foetoproteïne (merker primaire levertumor) normaal |
Normaal, behalve bij grote letsels: gestegen AF en gamma-GT Alfa-foetoproteïne normaal |
Normaal, behalve bij grote letsels: gestegen AF en gamma-GT Alfa-foetoproteïne normaal |
Normaal, behalve bij grote letsels: gestegen AF en gamma-GT Alfa-foetoproteïne normaal (bij maligne ontaarding wel gestegen!) |
Alfa-foetoproteïne gestegen (CAVE sporadisch gestegen bij chronische hepatitis, cirrose en ZS) |
HistoPatho |
Biliair / ziekte van Caroli / parasitair (echinococcus cyste) | Caverneuze hemangiomen Fibrose/sclerose mogelijk |
Lokale hyperplasie Dystrofische bloedvaten Fibreuze septa Geen ducti, wel uitgebreide ductulaire reactie Macroscopisch ~cirrose Regeneratienodules cirrotische lever kan lijken op FNH |
Weinig gedifferentieerd Geen ducti Niet omkapseld |
In normale lever (zeldzaam) Meestal gedacht aan meta Naaldbiopsie bij twijfel In cirrotische lever Dysplastische noduli Transformatie naar goed gedifferentieerd HCC (early) Neoangiogenese Dedifferentiatie (progressed) Vasculaire invasie & metastasering Verstoord reticulinepatroon ~ maligne transformatie |
Behandeling |
Geen behandeling nodig, tenzij symptomatisch (bloeding/surinfectie) of twijfel aanwezigheid vast weefsel → percutane aspiratie, chirurgische fenestratie |
Zelfs indien volumineus geen behandeling vereist Geruststelling patiënt Enkel resectie bij symptomen |
**Geen behandeling **Patiënt geruststellen |
Stop OC & anabole steroïden Nauwgezette follow-up Chirurgische resectie bij verhoogd risico op ontaarding: - volumetoename > 5cm - verwikkelingen - bij man |
Heelkundige resectie: < 5cm reseceerbaar **Transplantatie: **niet-reseceerbaar<5cm <3 letsels belangrijke cirrotische lever (in afwachting ablatie, chemo-embolisatie, radionucleïdetherapie…) Chemo/lokale therapie: >5cm niet-reseceerbaar (sorafenib - kinase inhibitor) |
Important
Elke cirrhosepatiënt 6-maandelijks screenen (3%/j ontaarding):
- echo
- alfa-foetoproteïnebepaling
- bij minste twijfel → MRI
Important
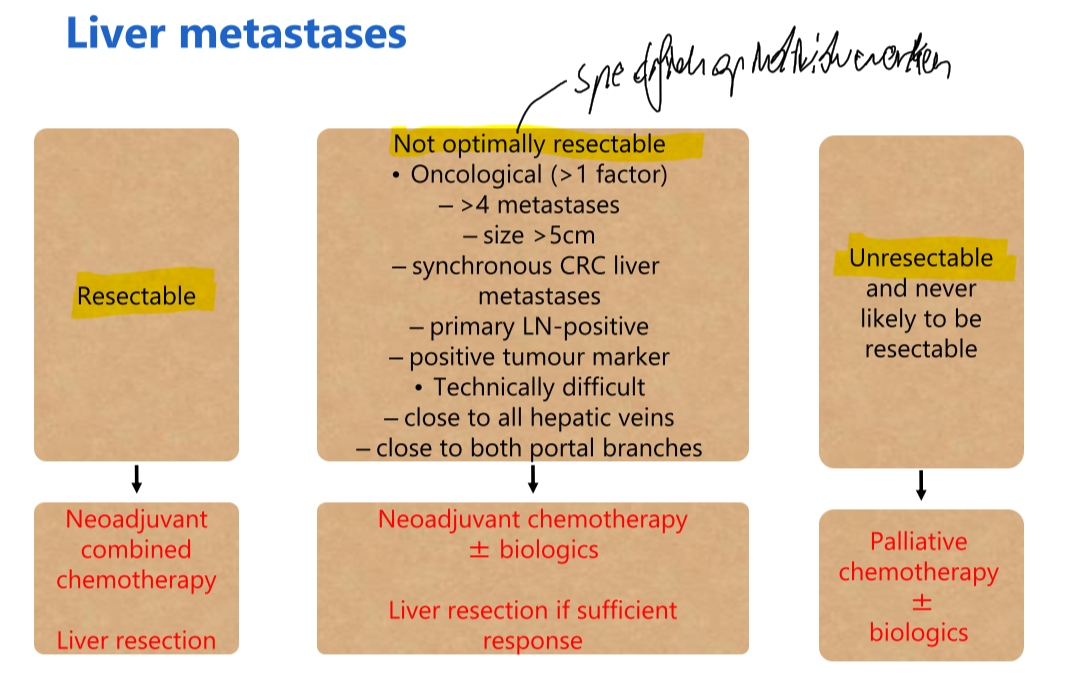
Levermetastase is meest frequente maligne tumor van de lever